
Nearly 500 active clinical trials. A 3.5-fold rise in annual trial starts in five years. A decisive pivot away from CBD isolates toward whole-plant, THC-containing medicines aimed at pain. The German authorisation of Vertanical’s Exilby (VER-01) in 2026 — the first high-THC, full-spectrum botanical ever to win pharmaceutical marketing authorisation — is not just a product launch. It is the visible leading edge of a cannabinoid clinical pipeline that has quietly tripled in a decade and is shedding its reputation as slow, single-molecule and indication-bound. This analysis, built on Cannamonitor’s Clinical Trials database (n = 1,305) and validated against workspace news, market reports and company disclosures, sets that approval against the pipeline it leads — including the parts still too young, too small and too skewed to match the headline.
Table of Contents
Three things to know before reading further. First, in four decades the licensed-cannabinoid shelf held just three names — and only one, Epidiolex, became a commercial force; Exilby is the fourth, and the first whole-plant THC medicine among them. Second, the clinical pipeline behind it is large but immature: nearly 500 trials are active, yet 56% sit at Phase I or II and barely 20% are late-phase. Third, the centre of gravity is shifting — full-spectrum, whole-plant formulations are now the single largest class in the active pipeline, overtaking the CBD isolates that dominated the completed evidence base, with late-phase THC concentrating exactly where Exilby is aimed: pain.
Exilby: the first whole-plant, high-THC medicine to clear a regulator
The approval is an inflection point because, for forty years, cannabinoid medicine meant three products and one hit. Dronabinol (Marinol), a synthetic THC isolate, was approved by the FDA in 1985 for chemotherapy-induced nausea and AIDS-related anorexia. Sativex (nabiximols), a balanced THC:CBD botanical from GW Pharma, followed in Canada (2005) and the United Kingdom (2010) for multiple-sclerosis spasticity. Epidiolex, GW’s purified cannabidiol isolate, arrived in 2018 for rare childhood epilepsies. Of the three, only Epidiolex became a commercial force, crossing $1.1bn in sales in 2025 and accounting for roughly a quarter of Jazz Pharmaceuticals’ revenue.
Exilby breaks the pattern on two fronts at once. It is high-THC and full-spectrum — a standardised whole-plant extract rather than an isolate or a balanced blend — and it targets chronic low-back pain of a radicular, neuropathic character. No botanical of this kind had previously cleared a pharmaceutical regulator, and it did so in pain, the indication GW itself never cracked.
The evidence base is unusually deep for the field. Vertanical won approval not on a single study but on a coherent Phase III package: a placebo-controlled pivotal trial establishing efficacy, long-term safety and — decisive for a THC medicine — no evidence of dependence or withdrawal; an active-controlled head-to-head against opioids (384 patients) reporting superior pain reduction and better gastrointestinal tolerability; and a third, larger Phase III (810 patients) now registered to confirm the effect in a neuropathic-dominant population and align with the United States pivotal programme. The two completed trials enrolled more than 1,200 patients — the kind of late-phase maturity the wider pipeline still lacks.
The commercial logic is direct. Germany writes on the order of 18m opioid prescriptions a year; a non-opioid analgesic with a clean dependence profile has an obvious substitution narrative. Launch is expected around September 2026, with a United States Phase III readout in 2027 and an NDA anticipated in 2028; Exilby already holds FDA Breakthrough Therapy Designation. A quieter structural advantage underpins it: licensed pharmaceuticals secure reimbursement that remains elusive for dispensed cannabis — tellingly, Germany is cutting statutory reimbursement of dried flower even as licensed products retain a route to it.
The pipeline tripled with ~500 active trials, but few reach late stage
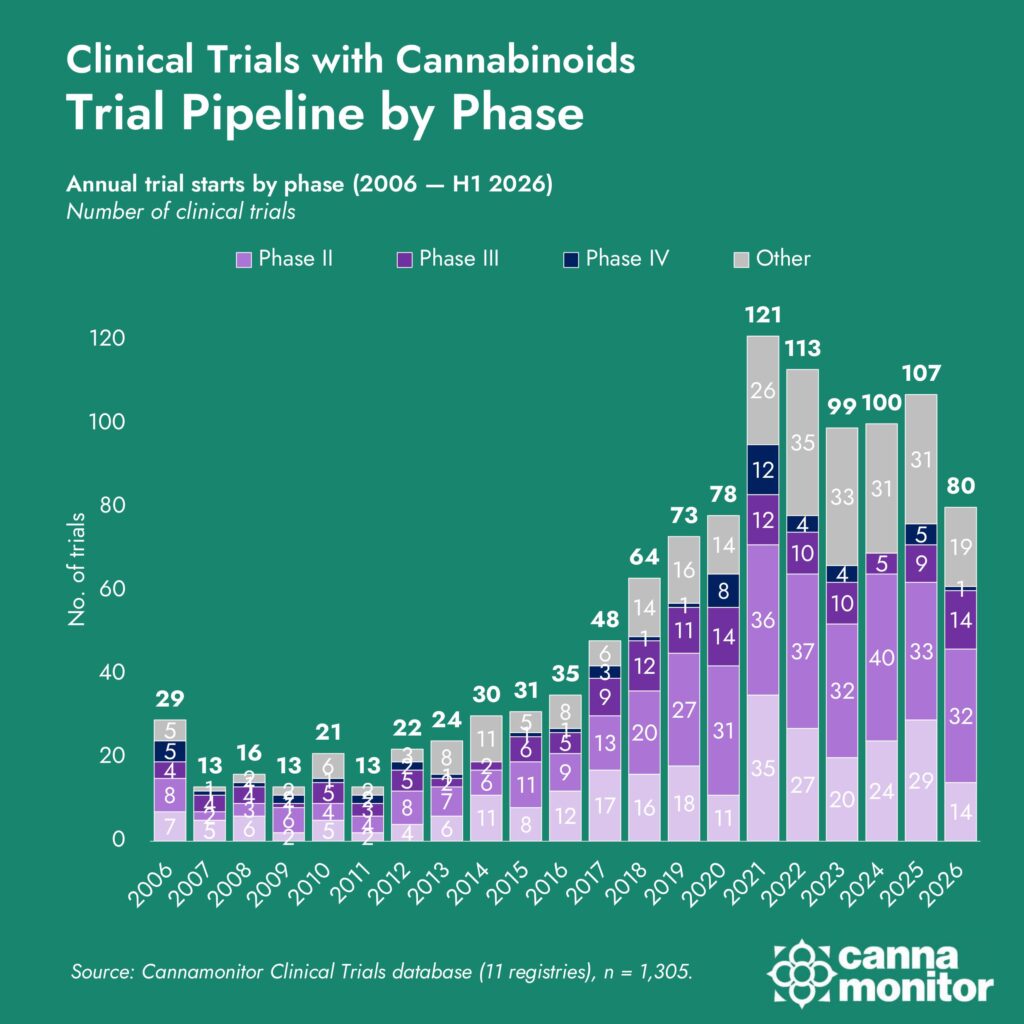
Behind the single approval sits a body of clinical activity that has expanded relentlessly. Annual cannabinoid trial starts climbed from about 29 in 2006 to a peak of 121 in 2021 — roughly one new human study every three days — and have held near 100 a year since. Cumulatively, the field has gone from 132 trials before 2010 to 361 across 2010–2019 and 698 in 2020–2026: a 3.5-fold rise in annual starts between 2016 and 2021 alone. At any given moment today, nearly 500 trials are active (483, of which 306 are actively enrolling).
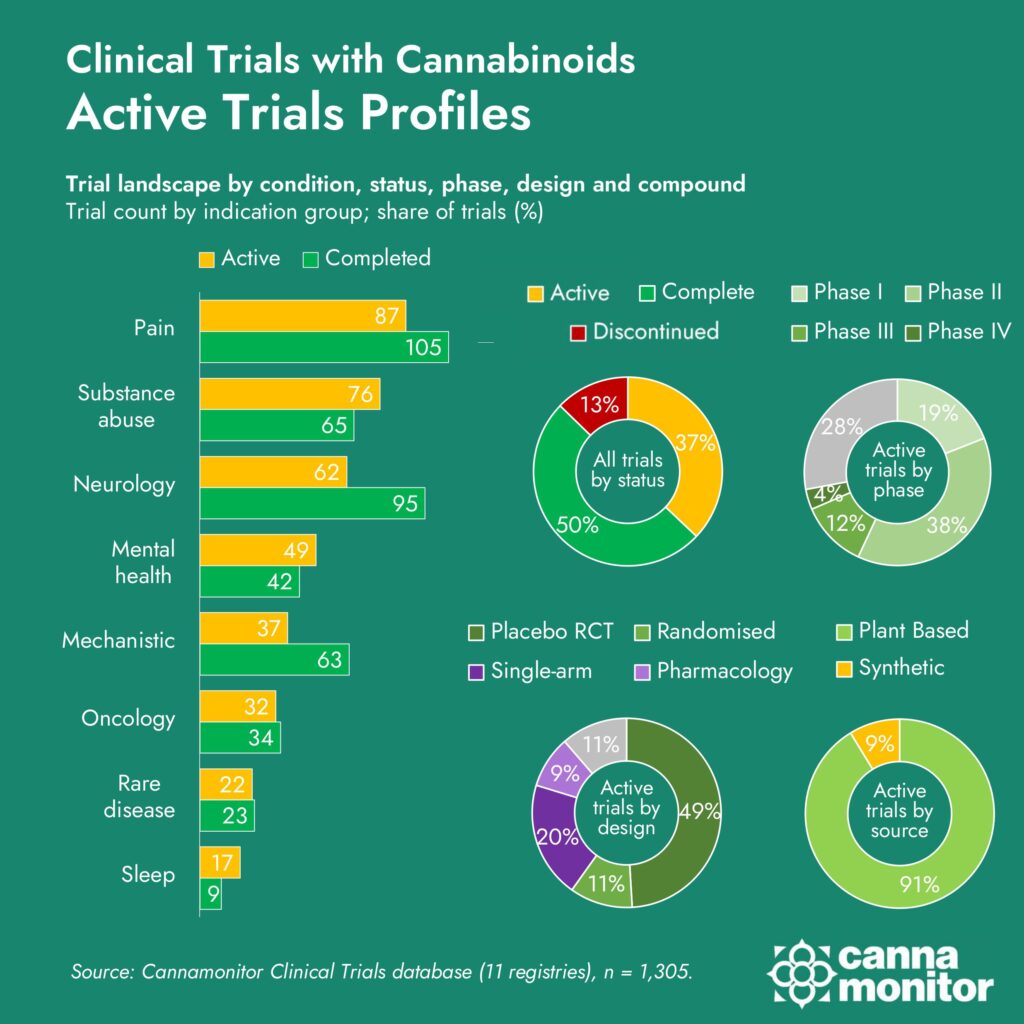
But the pipeline is younger and smaller than the headline count suggests. Some 56% of all trials sit at Phase I or II; only 20% are late-phase (III/IV), and late-phase is thinner in the active pipeline (15%) than among completed studies (22%) — the pivotal wave is still building. What the pipeline does not lack is rigour: the charge that the evidence is merely observational does not hold, with real-world and observational work just 3% of the total and 49% placebo-controlled randomised trials by design. The genuine gap is scale, duration and late-phase maturity, not method.
The composition of that activity is also skewed. Much of the field is still not front-line therapeutics: substance-use research (24%) and healthy-volunteer or mechanistic work (11%) together make up 35% of all trials, ahead of pain (21%), neurology (16%) and mental health (13%). That skew is heavily North-American: substance-use and mechanistic studies account for 42% of United States trials and 37% of Canadian ones, against 14% in the United Kingdom and 9% in Israel — a signature of NIH- and NIDA-driven funding priorities rather than therapeutic intent. Across the panel’s other axes, the active pipeline reads the same way: it skews early-phase and still-enrolling, leans on interventional, placebo-controlled designs rather than observational ones, and is dominated by plant-derived formulations over synthetic molecules.
Clinical trial pipeline by phase (annual starts, 2006—H1 2026)
Active trials profiles (indication, status, phase, design, source)
Full-spectrum overtakes CBD as late-phase THC focuses on pain
Late phase trials by condition (active Phase III/IV: THC vs CBD)
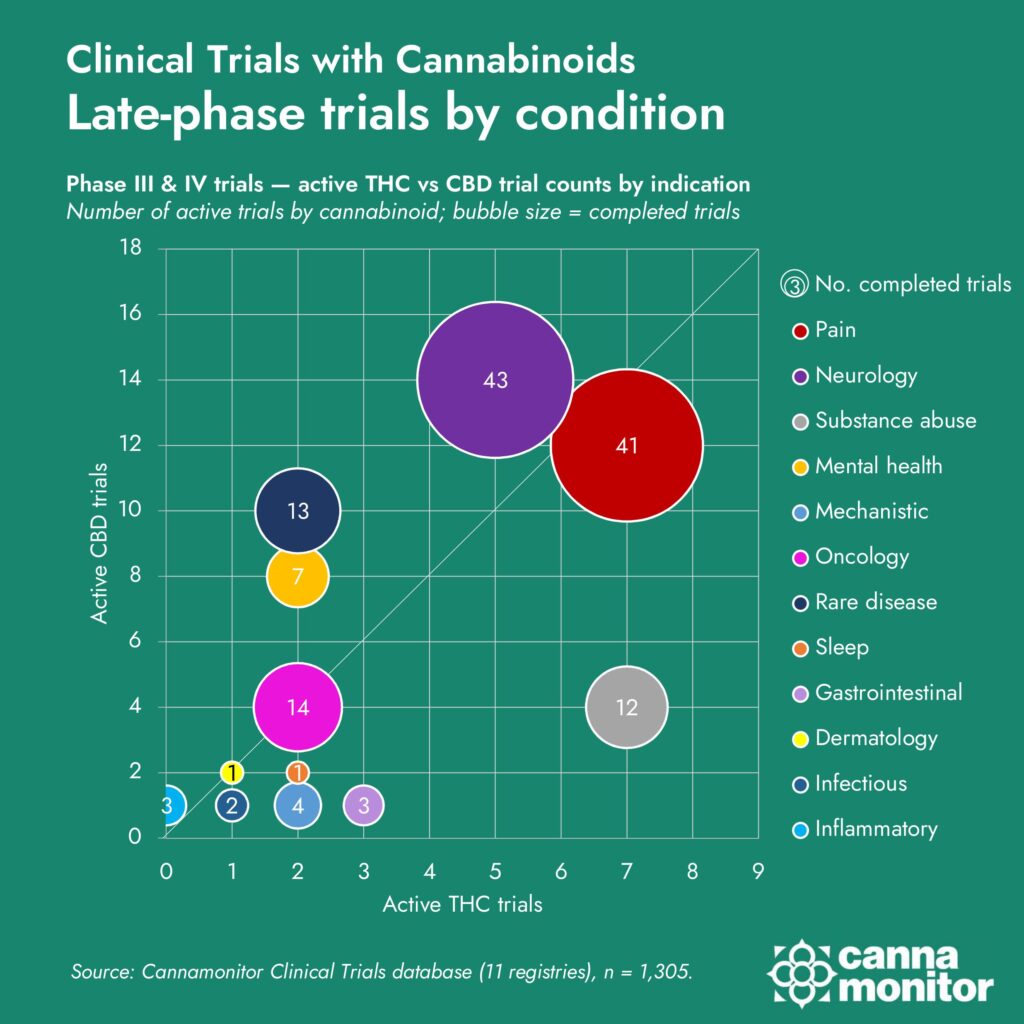
Late phase trials by condition (active Phase III/IV: THC vs CBD)
The most important signal in the data is a shift in where late-phase evidence is concentrating. Early-stage work still contains a large share of substance-use and mechanistic studies, but when you isolate Phase III/IV activity the field looks more clinically “serious”: late-stage programmes cluster in the indications where regulators and payers will demand hard efficacy and safety data — and where Exilby is positioned.
The formulation mix is turning decisively. The completed evidence base is CBD-led — CBD-only formulations were the largest defined class at 26%, full-spectrum at 25%, THC-only at just 15% and balanced products at 10%. The active pipeline inverts that order: full-spectrum, whole-plant formulations have risen to 34%, overtaking CBD-only (33%) to become the single largest class — precisely the Exilby model — while THC-only has slipped to 11% and balanced to 2%. Crucially, in late-phase (III/IV) active trials, THC is concentrating in pain and substance use, the indications where its pharmacology is best evidenced.
A regulatory tailwind reinforces the turn. In the United States, FDA-approved and state-licensed medical cannabis moved from Schedule I to Schedule III, effective 28 April 2026, easing §280E tax treatment and — importantly for researchers — legal sourcing of study material; a broader DEA hearing runs 29 June–15 July 2026. The controlled-substance friction that long throttled THC research is easing just as the pipeline leans into it.
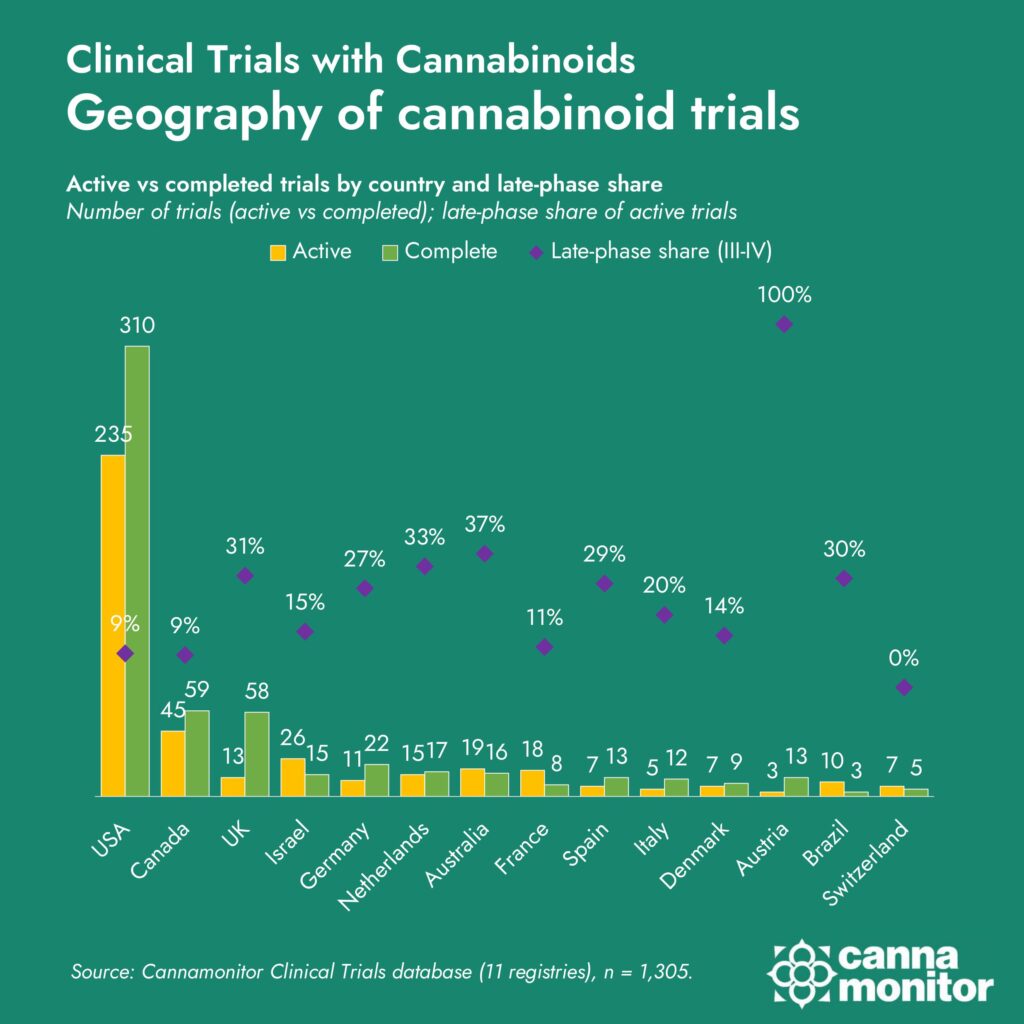
That turn is also uneven across geographies, and the late-phase weight sits where whole-plant THC programmes have advanced furthest. The United States is tagged in 644 trials, followed by Canada (122), the United Kingdom (102), Germany (56) and Israel (55). The United States runs the largest but earliest-stage share; Europe and Australia carry proportionally more late-phase work — the same regions, led by Germany, where the pain-first, full-spectrum model behind Exilby has cleared or is nearing the clinic.
A crowded biotech field circumventing GW's patent wall
Beyond Vertanical, more than 50 companies are developing cannabinoid investigational products, and almost all are defined by a single strategic problem: how to navigate the intellectual-property estate GW Pharma (now Jazz) built around Epidiolex — method-of-use and formulation patents running to 2035 and beyond, orphan and data exclusivities, and active litigation against generic challengers. Because no one can patent CBD or THC as molecules, developers take one of four observable routes around that wall: a known molecule in a new indication (for example Cardiol Therapeutics in pericarditis, Ananda Pharma in endometriosis pain); a new synthetic molecule free of scheduling (Corbus, Aelis Farma, Skye Bioscience); a new form or combination of a known cannabinoid (Zynerba’s transdermal gel, Incannex’s fixed-dose combination); or the full-spectrum botanical as the drug itself, the route Vertanical has now proven can succeed.
It is also a late-stage graveyard. Three of the most-watched programmes ended in disappointment: Corbus missed every Phase III and Phase IIb endpoint across its lenabasum programme; Zynerba/Harmony saw its Phase III RECONNECT fail in 2025; and Canada’s Tetra Bio-Pharma entered voluntary bankruptcy in 2023. Meanwhile capital is rotating towards CB1 inhibition for obesity — a pharma-grade, non-plant frontier that competes with botanical pain programmes for investment.
That backdrop is what gives the Exilby story its edge. Its approval is simultaneously a vindication of the full-spectrum, pain-first thesis and a standout against a field where most cannabinoid drug bets have stalled. The data shows a pipeline that has tripled in size, matured unevenly, and pivoted hard toward whole-plant THC for pain — and a licensed route that, after two decades of three products and one hit, has finally produced a fourth. The open question is no longer whether a whole-plant medicine can clear a pharmaceutical regulator, but how many of the 50-plus programmes now in the pipeline can convert that proof of concept into the late-phase evidence the field still mostly lacks.
Sources & method. Analysis built on Cannamonitor’s Clinical Trials database (1,305 trials), validated against news and market reports including Jazz Pharmaceuticals’ FY/4Q25 results (Epidiolex $1.1bn).